 Sen Ma
Sen Ma Yan Gao
Yan Gao Liangyu Zhao
Liangyu Zhao Wenze Sui
Wenze Sui- School of Physical Education, Shandong University, Jinan, China
Background: Quality of Life (QoL) is a crucial multi-dimensional structure in the development process of adolescents. As a key topic in adolescent research, existing achievements all indicate that participating in physical activities can improve the QoL of adolescents. However, the underlying mechanisms—the mediating role of anxiety and the underlying gender differences—remain insufficiently understood.
Purpose: This study investigates the mechanisms by which adolescent physical activity influences QoL. Specifically, it examines the mediating role of anxiety and explores gender as a moderating factor. A multidimensional analysis of QoL outcomes is also conducted to provide a more nuanced understanding.
Methods: We analyzed cross-sectional data from 9,504 adolescents across 17 cities in Shandong Province, China. The collected data were statistically analyzed using SPSS 27.0. Build a moderated mediation model using the PROCESS macro of SPSS.
Results: (1) There is a significant positive correlation between teenagers’ participation in sports and their QoL (β = 4.243, p < 0.01). (2) Anxiety plays a key mediating role between teenagers’ participation in sports and their QoL (β = 0.594, p < 0.05). (3) Gender plays a significant positive moderating role between adolescent sports participation and QoL (β = 0.781, p < 0.01). (4) Gender plays a significant positive moderating role between anxiety and QoL (β = 1.214, p < 0.05). (5) Gender plays a significant positive moderating role in the relationships between anxiety and living environment (β = 0.536, p < 0.01).
Conclusion: Teenagers’ participation in sports can directly or indirectly improve their QoL by reducing anxiety. Meanwhile, gender plays a moderating role in it. Furthermore, gender plays a significant moderating role in the relationships between anxiety and psychosocial function, anxiety and physical and mental health, anxiety and living environment, and exercise participation and physical and mental health. These findings emphasize the importance of adopting gender-specific strategies in physical intervention measures to improve the QoL of adolescents.
1 Introduction
According to the definition given by the World Health Organization (WHO), Quality of Life (QoL) encompasses an individual’s perception of their living standards and status within the realm of their life culture and values, as well as their life goals, future life, living standards and concerns (1). Among adolescents, QoL serves as a critical indicator of developmental well-being, shaped by both maturational processes and situational life events, and represents a key outcome in public health and healthcare promotion initiatives (2, 3). The number of adolescents worldwide has soared to a record level, reaching 1.3 billion, which constitutes approximately one-sixth of the global population. This number is expected to keep rising through 2050, particularly in low- and middle-income nations, where nearly 90% of individuals aged 10 to 19 reside (4).
Adolescent QoL not only influences immediate outcomes such as academic performance and social adaptability (5), but also exerts long-term effects on future mental health and psychosocial functioning (6). For this population, QoL extends beyond physical health and scholastic achievement to include psychological well-being (7), social adaptation, and overall life satisfaction (5, 8). In the Chinese research context, a well-established multidimensional QoL model for adolescents incorporates four core domains: psychosocial functioning, physical and psychological health, environmental quality, and satisfaction with life (9). Numerous scholars emphasize that identifying and understanding the determinants of adolescent QoL is essential for developing targeted intervention strategies (10). Recent efforts in this field have focused on the early detection of risk and protective factors, the design of evidence-based interventions, and the assessment of both short- and long-term benefits (11, 12). Nevertheless, from a personalized intervention standpoint, there remains a pressing need to develop and evaluate more effective strategies that can be tailored to adolescents across different ages, sexes, and sociocultural backgrounds. Therefore, this study aims to investigate the key mediating role of anxiety in the relationship between physical activity and adolescent well-being, while also evaluating the potential moderating effect of gender on this mediation pathway. Moreover, a multidimensional assessment of QoL has enhanced the overall understanding of the topic.
1.1 The relationship between physical activity and quality of life
Among the most compelling and widely studied protective factors is physical activity —an area of growing scholarly attention in recent years (13). Adolescence represents a pivotal transitional stage in personal development (4), during which both consistent physical activity and psychological stability play essential roles (14). More and more evidence shows that improving the level of physical participation has significant benefits for the physical and mental health of teenagers (15). Conversely, low levels of participation have been linked to increased risk for psychological disorders and diminished QoL (16–18). Engaging in regular physical activity not only enhances physical fitness and somatic health (15), but also improves subjective well-being and life satisfaction by fostering a more positive bodily self-perception (19). As such, physical activity represents a crucial avenue for promoting holistic adolescent development and elevating QoL across multiple dimensions.
While preliminary evidence suggests that physical activity may positively influence both physical and psychological well-being, as well as overall quality of life among adolescents (20), current research remains insufficient in elucidating the underlying mechanisms driving these effects. A particularly important but under-researched mechanism is the mediating role of anxiety within this relationship. Specifically, there is a lack of empirical studies that rigorously examine and confirm this mediating pathway, which limits the ability to quantitatively determine the degree to which anxiety accounts for the beneficial impact of physical activity on adolescent quality of life. Examining this mechanism is especially pertinent during adolescence—a critical developmental period for establishing emotional and social competencies that are foundational to mental health. Understanding how physical activity improves quality of life through anxiety mitigation carries significant theoretical and practical implications for designing targeted, evidence-based interventions to promote youth health.
1.2 The mediating role of anxiety
Adolescents today face multiple challenges, including academic pressure, social difficulties, and the complexities of physical and mental development, leading to a significant decline in time spent engaging in physical activity (21), and increasingly prominent mental health issues (22). It is estimated that around 14% of the global population between the ages of 10 and 19 is impacted by mental health disorders (23), many of which go unrecognized and receive no treatment. Young people facing such psychological challenges are at a higher risk of encountering social marginalization, prejudice, and stigmatization—which may discourage them from accessing support—as well as struggles in academic settings, engagement in dangerous activities, physical health complications, and breaches of their fundamental human rights (24). Anxiety, as one of the most common psychological problems among adolescents, It is estimated that 4.4% of individuals between the ages of 10 and 14, and 5.5% of those aged 15 to 19, are impacted by anxiety disorders (23). Anxiety not only directly affects their mental health, but may also indirectly influence their QoL (QoL) through a series of psychological and behavioral responses (25, 26). The elevated levels of life stress associated with anxiety disorders may impair psychological health and foster a progressively isolated and sedentary lifestyle (27). Adolescents with high levels of anxiety often exhibit lower life satisfaction and social competence, as well as more pronounced psychological and behavioral issues (28).
Physical exercise is not only a fundamental component of physical health, but also plays a vital role in promoting mental and emotional well-being, ultimately contributing to an enhanced overall QoL (29). Regular participation in physical activities stimulates the brain’s natural release of endorphins—neurochemicals that foster social bonding, reduce pain perception, and improve emotional state (30, 31). Consequently, individuals are likely to experience diminished feelings of anxiety and sadness. Meanwhile, current meta-analytic evidence derived from adolescent and young adult cohorts suggests that consistent engagement in physical activity and a variety of exercise modalities may play a role in mitigating symptoms of depression and anxiety (29, 31). Research from Turkey demonstrates that consistent engagement in sports activities is significantly associated with reduced levels of social anxiety. Higher levels of physical exercise contribute to the reduction of anxiety symptoms and help alleviate the detrimental effects associated with psychological disorders (32).
According to Social Cognitive Theory (SCT), within the domain of sports, sustained participation can significantly enhance adolescents’ self-efficacy during critical developmental periods, particularly in domains such as bodily control, overcoming athletic challenges, and regulating emotional responses—ultimately contributing to a substantial reduction in anxiety (33). Therefore, physical activity serves as a key cognitive-emotional mechanism for alleviating anxiety through the enhancement of both sport-related and emotion-regulation self-efficacy. Moreover, Self-Determination Theory (SDT) posits that engaging in appropriate forms of physical activity effectively fulfills adolescents’ fundamental psychological needs (34). When these essential needs are satisfied, physical activity fosters the development and maintenance of intrinsic motivation, thereby promoting greater willingness and consistency in participation, which establishes a reinforcing cycle that amplifies its enduring efficacy in anxiety reduction (35). Collectively, these theoretical perspectives provide a robust foundation for the central hypothesis of this study: that anxiety mediates the relationship between physical activity engagement and QoL. On the other hand, according to the Hypothalamic–Pituitary–Adrenal (HPA) axis theory, physical activity can reduce the secretion of cortisol by regulating the activity of the HPA axis, thereby alleviating anxiety (36). There is clear neuroendocrine evidence supporting the inhibitory effect of physical activity on anxiety (e.g., normalization of HPA axis function), which provides biological plausibility for the mediating pathway “physical activity → anxiety reduction → QoL improvement” (37, 38).
1.3 The moderating role of gender
In addition, it is worth noting that adolescents of different genders, ages, and family backgrounds may exhibit significant differences in physical activity, anxiety levels, and QoL (39, 40). Given that gender-based disparities emerge across multiple domains—including patterns of physical activity, the prevalence of anxiety disorders, and subjective perceptions of QoL (41)—this study integrates gender as a pivotal moderating variable within the mediation framework. Drawing upon Gender Role Theory, the formation of distinct gender roles during adolescence heightens societal expectations regarding gender-specific behaviors and emotional expression (42). For instance, girls are often socially permitted to exhibit anxiety but face greater external judgment, whereas boys are typically expected to mask their emotions while managing heightened performance pressures (43). These divergent socialization processes may shape adolescents’ motivation to engage in physical activity, their sensitivity to and expression of anxiety, and the dimensions of QoL they value most (42, 44). Accordingly, we posit that gender not only influences adolescents’ participation in physical activity, their anxiety levels, and their perceived QoL, but also modulates the degree to which physical activity functions as a pathway for alleviating anxiety and enhancing overall well-being.
Additionally, the study explored a range of demographic factors—including age, family socioeconomic status, and residential context—that may exert influence on the primary variables (45). Crucially, drawing upon gender role theory and developmental research on adolescence, these control variables may exhibit differential effects across genders with respect to participation in physical activity, levels of anxiety, and subjective perceptions of QoL. Consequently, demographic control variables were incorporated into the analytical framework to account for their potential moderating influence when examining the role of gender.
In view of the previously described context, this study centers on adolescents as the focal population and establishes a moderated mediation model. The following research hypotheses are proposed:
H1: There is a positive relationship between adolescent physical activity and QoL.
H2: Anxiety functions as a mediator in the relationship between adolescent physical activity and QoL.
H3: Gender moderates the association between adolescent physical activity and QoL.
H4: Gender serves as a moderator in the relationship between adolescent physical activity and anxiety.
H5: Gender acts as a moderating factor in the relationship between anxiety and QoL.
The hypothesized model is presented in Figure 1.
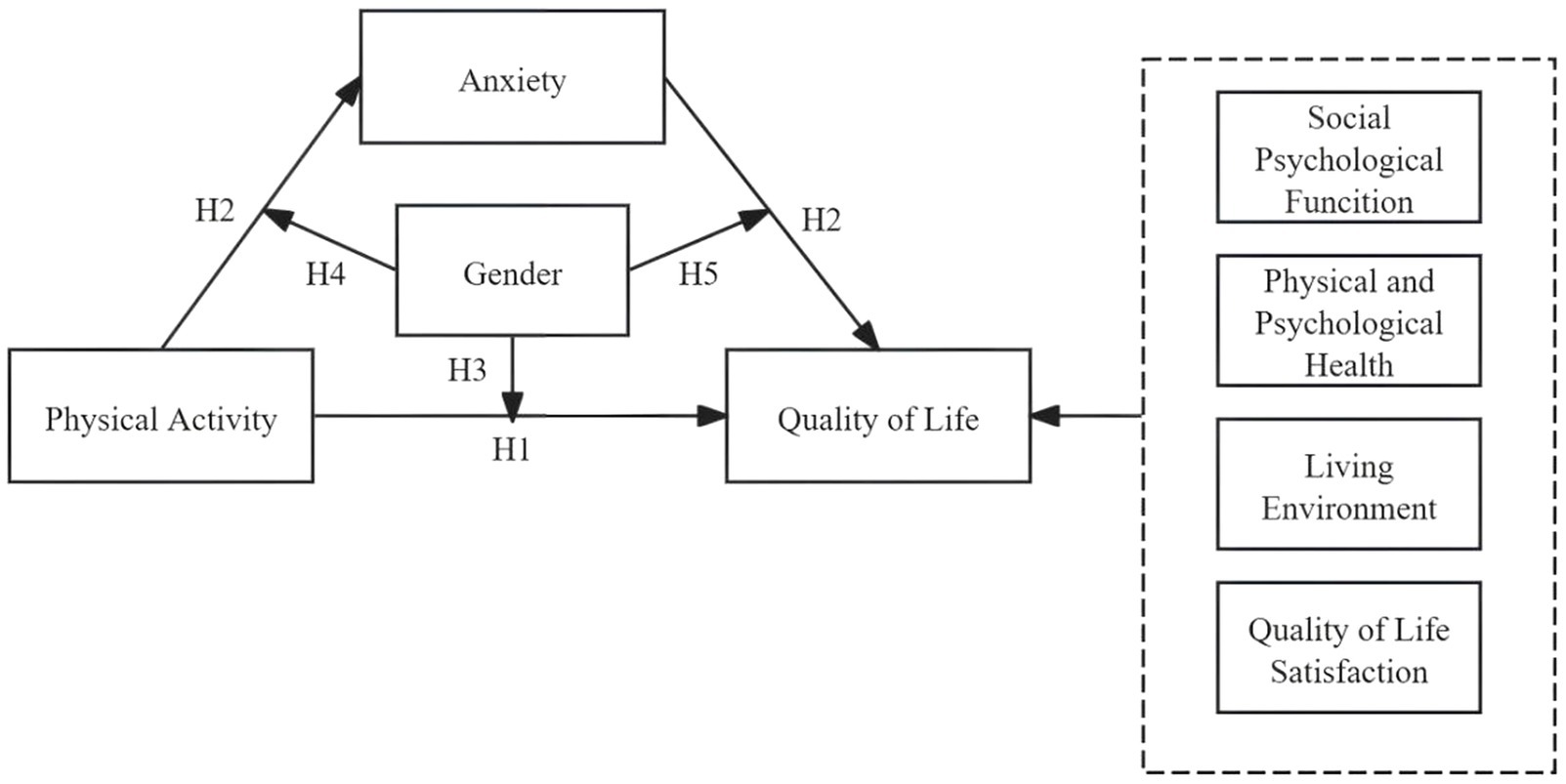
Figure 1. Theoretical hypothesis model.
2 Methodology
2.1 Participants and procedures
This study was conducted in accordance with the guidelines of the Declaration of Helsinki. All procedures involving human participants were approved by the Ethics Committee of Shandong University (20180517). This study adopted the probability Proportional sampling (PPS) method. Participants were randomly selected from 186 middle and high schools in 16 prefecture-level cities (Jinan, Qingdao, Zibo, Zaozhuang, Dongying, Yantai, Weifang, Jining, Taian, Weihai, Rizhao, Linyi, Dezhou, Liaocheng, Binzhou, Heze) of Shandong Province during 2020–2021. The target sample consisted of adolescents aged 12 to 18 years. The demographic characteristics of the participants are detailed in Table 1. Both the research participants and their parents signed the written informed consent form. The data collection process strictly adheres to standardized protocols: researchers who have undergone two rounds of standardized training provide on-site guidance for students to complete the questionnaire filling. The entire research process adheres to the principles of anonymization and confidentiality.
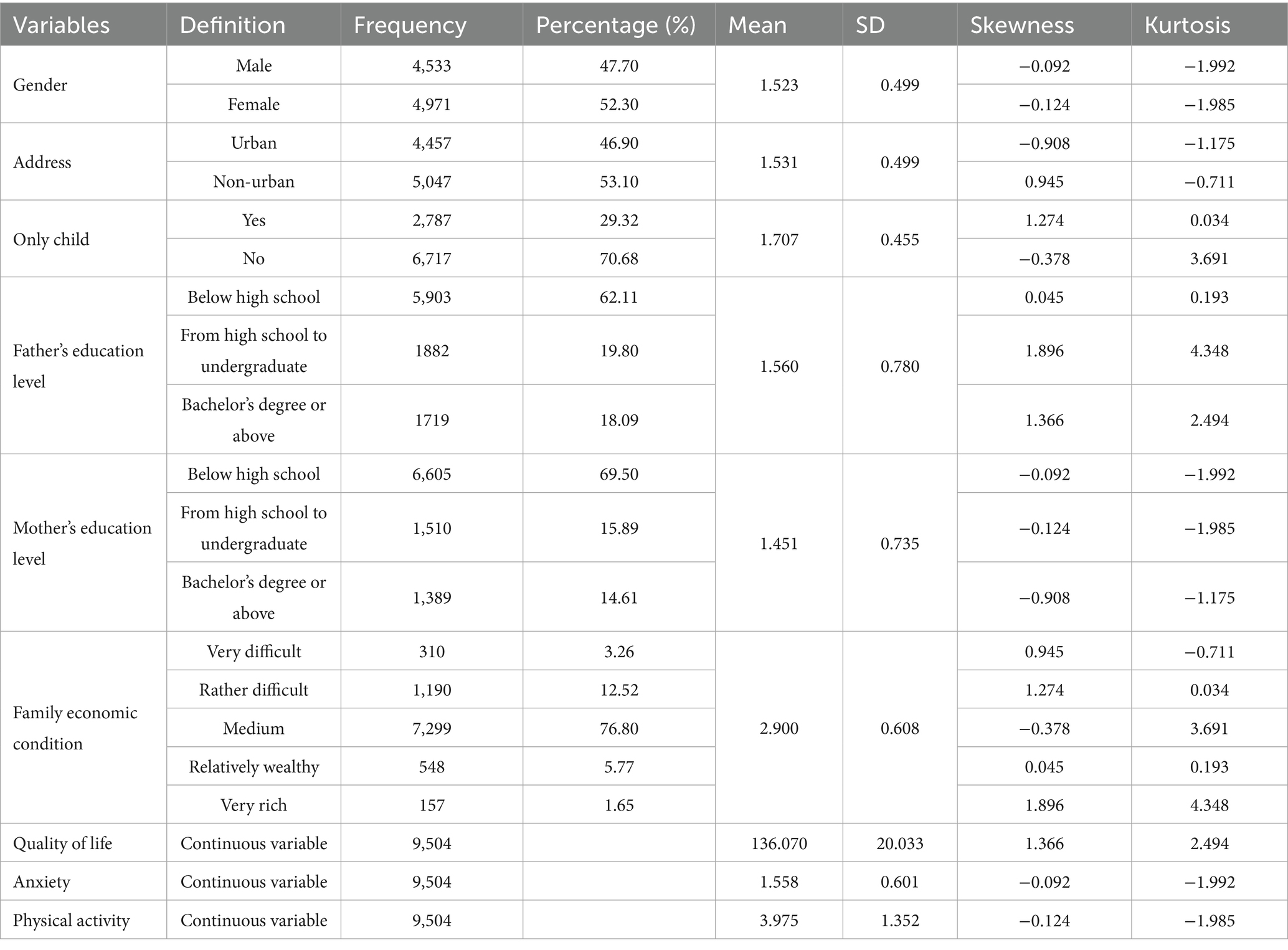
Table 1. Sociodemographic characteristics of the participants and descriptive statistics for main variables.
2.2 Measures
2.2.1 Physical activity questionnaire for adolescents (PAQ-A)
This study assessed the physical activity levels of adolescents using the revised Physical Activity Questionnaire for Adolescents (PAQ-A), originally developed by Li Xin et al. (46). This scale consists of nine items designed to evaluate adolescents’ daily physical activity levels over the past week. It also investigates whether any unusual circumstances arose during this period that could have affected their usual participation in physical activities. All questions are evaluated based on a five-point Likert scale. The overall score is determined by averaging the values of all items, where higher scores signify increased physical activity levels. Specifically, a score exceeding 3 indicates high physical activity levels, scores between 2 and 3 suggest moderate participation, and scores below 2 signify low involvement. To test the reliability and validity of SCL-90, exploratory factor analysis was used to test the validity of the scale (KMO = 0.868, p = 0.000), and Cronbach’s alpha was used to test its reliability (Cronbach’s alpha = 0.930) (47).
2.2.2 The QoL scale for children and adolescents (QLSCA)
The QoL Scale for Children and Adolescents (QLSCA), developed by Wu Hanrong and colleagues, was employed to assess the QoL among adolescents (10). The QLSCA comprises 49 items, encompassing four main domains: physical and mental health, psychosocial functioning, living environment, and satisfaction with QoL. It covers 13 particular aspects, such as the interaction between teachers and students, relationships among peers, the dynamics within parent–child interactions, competence in learning along with associated attitudes, one’s self-perception, overall physical health, experiences of negative emotions, perspectives on homework, the ease of daily living, chances for participating in activities, athletic proficiency, and a sense of personal satisfaction. Each item on the scale is rated on a four-point Likert scale (1 = never; 2 = rarely; 3 = often; 4 = always), where lower scores indicate a poorer QoL and higher scores indicate a better QoL. The scale contains 13 negatively worded items. The total score is calculated by summing the scores for all items. To test the reliability and validity of SCL-90, exploratory factor analysis was used to test the validity of the scale (KMO = 0.965, p = 0.000), and Cronbach’s alpha was used to test its reliability (Cronbach’s alpha = 0.939) (48).
2.2.3 The symptom checklist-90 (SCL-90)
Anxiety levels were assessed through the Symptom Checklist-90 (SCL-90), a psychological measurement instrument created by Derogatis and his team (49). The SCL-90 consists of 90 items across 9 factors, with item content derived primarily from psychopathological symptomatology. It encompasses a wide range of domains, including sensory experiences, cognition, affect, behavior, interpersonal relationships, daily habits, diet, and sleep. It is commonly used to evaluate mental health status and behavioral problems. This study specifically employed the Anxiety subscale, one of the nine factors, comprising 10 items (items 2, 17, 23, 33, 39, 57, 72, 78, 80, and 86). These items indicate psychological symptoms and experiences with a clinical association to anxiety disorders. Each item is scored on a four-point scale. The final score is calculated as the average across all items. A score above 2 implies the existence of anxiety symptoms, whereas a score of 2 or less signifies their nonexistence. To test the reliability and validity of SCL-90, exploratory factor analysis was used to test the validity of the scale (KMO = 0.948, p = 0.000), and Cronbach’s alpha was used to test its reliability (Cronbach’s alpha = 0.911) (50).
2.2.4 Socio-demographic variables
This study included several socio-demographic factors as control variables, including gender, family structure, parental education level, household economic status, and residential location. Gender served as a moderating variable and was coded as a dummy variable (1 = male, 2 = female). Family structure was defined by whether the adolescent was an only child. Only-child status was coded as 1; non-only-child status was coded as 2. Parental education level was measured based on the highest level of education attained (excluding adult education), coded as follows: below high school = 1, high school to undergraduate level = 2, above undergraduate = 3. Household economic status was categorized into five levels: 1 = very poor, 2 = relatively poor, 3 = average, 4 = relatively affluent, 5 = very affluent. Based on the actual construction situation, the location of the residence is classified as urban (code 1) or non-urban (code 2).
2.3 Statistical analyses
Initially, the dataset was examined to confirm its authenticity, validity, and alignment with the study’s requirements. A power analysis performed with G*Power 3.1 revealed that at least 103 participants were required to detect the intended effect size with 80% statistical power and a significance threshold of.05. The obtained sample size of 9,504 clearly exceeded this minimum criterion (51). Subsequently, the required variables were extracted and documented using the specified tools. All analyses were conducted using SPSS 27.0 software (IBM SPSS Inc., Chicago, USA). The statistical methods employed included evaluations for common method bias, descriptive statistics, correlation analysis, and analysis of variance (ANOVA). To remove the impact caused by the dimensionality differences in the independent variable, all variables were standardized before performing the mediation analysis. To investigate the mediating influence of anxiety in the relationship between adolescents’ physical activity and QoL, Model 4 of the SPSS PROCESS macro was utilized. A bias-corrected bootstrap percentile approach was applied to calculate 95% confidence intervals (CIs). If the CI for a path coefficient did not encompass zero, the mediating effect was deemed statistically significant. Lastly, Model 59 of the PROCESS macro was applied to evaluate the moderating role of gender within the mediation framework.
3 Results
3.1 Common method bias test
The Harman single-factor test was employed to assess the presence of common method bias (52). The analysis extracted 12 factors with eigenvalues exceeding 1, where the largest factor explained 21.16% of the total variance, which is substantially lower than the 40% criterion. Consequently, these findings suggest that common method bias does not pose a substantial issue in this study.
3.2 Descriptive statistics
Table 1 displays the descriptive statistical measures, inter-variable correlations, and reliability estimates for the variables under investigation. Analysis revealed that the distribution of all variables deviated from normality, as evidenced by kurtosis and skewness values that surpassed the conventional thresholds (53). The sample comprised a total of 9,504 participants, among whom females accounted for a slightly larger proportion (52.30%) than males (47.70%). Over half of the participants originated from non-urban regions (53.10%), and the majority were not only children (70.68%). Furthermore, most participants reported that their families had a moderate economic situation (76.80%), and their parents generally possessed relatively low levels of educational attainment, with 62.11% for fathers and 69.50% for mothers.
3.3 Analysis of variance
The results of the analysis of variance of the main variables are shown in Supplementary Table 1. Female students scored significantly lower than male students in terms of physical activity and QoL (p < 0.01), but exhibited significantly higher scores in anxiety (p < 0.01). Furthermore, teenagers residing in urban areas exhibited markedly greater levels of physical activity and QoL compared to their counterparts in non-urban settings (p < 0.01) and significantly lower anxiety scores (p < 0.01). Regarding only-child status, no notable difference was found in QoL scores between children without siblings and those with siblings (p > 0.05). However, children without siblings demonstrated markedly higher physical activity levels and reduced anxiety levels in comparison to children with siblings (p < 0.01). In terms of parental education, adolescents whose parents have completed high school, undergraduate, or higher levels of education showed markedly higher scores in QoL and physical activity, as compared to those whose parents did not finish high school (p < 0.01). In contrast, they had significantly higher anxiety scores. Finally, with respect to family economic condition, scores for QoL and physical activity increased with improvements in economic conditions, while anxiety scores decreased, all showing statistically significant differences (p < 0.01).
It should also be emphasized that, with the exception of family economic condition, the remaining control variables demonstrate limited clinical significance in explaining the observed variations in the outcomes (η2 < 0.015). Conversely, family economic condition exhibited a moderate effect in explaining variations in quality of life (η2 = 0.049), representing roughly 4.9% of the total variance. It indicates that there is a meaningful relationship between the family economic condition and an individual’s QoL (See Supplementary Table 2).
An analysis of variance was conducted for the four dimensions of QoL. As shown in Figure 2, significant differences based on gender were evident in the subsequent dimensions: Physical and Psychological Health (F = 13.445, p < 0.01), Living Environment (F = 144.611, p < 0.01), and QoL Satisfaction (F = 82.158, p < 0.01), with males scoring higher than females. However, no significant gender difference was observed in Social Psychological Function (F = 3.19, p = 0.074).
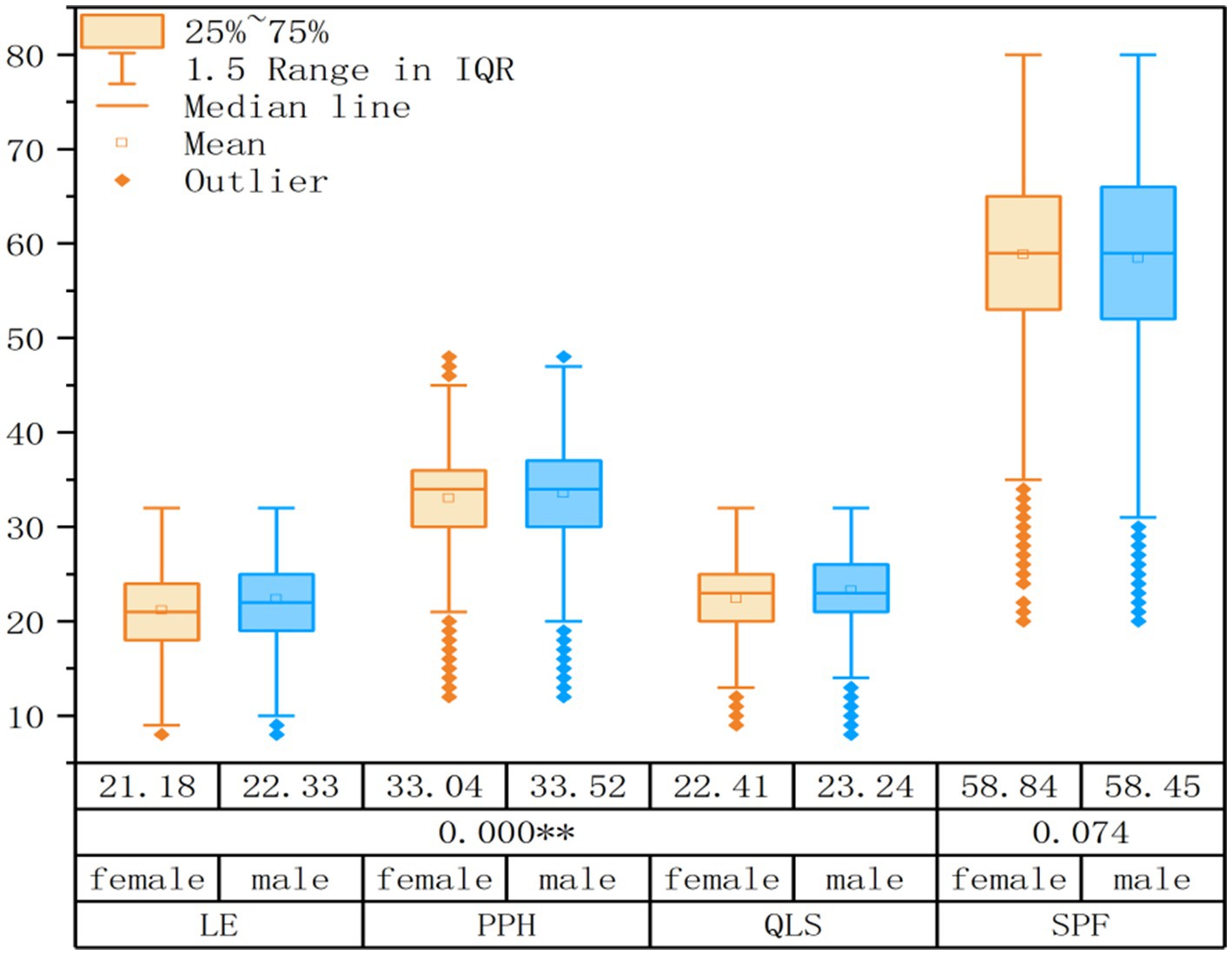
Figure 2. Multi-dimensional box plot of quality of life. SPF, Social Psychological Function; PPH, Physical and Psychological Health; LE, Living Environment; QLS, Quality of Life Satisfaction.
3.4 Correlation analysis
The correlation analysis results for the key variables are summarized in Table 2. The mean values of the key variables are summarized below: QoL (136.070 ± 20.033), adolescent physical activity (3.975 ± 1.352), and anxiety (1.558 ± 0.601). Pairwise correlations indicated statistically significant relationships: QoL showed a positive association with physical activity (R = 0.298, p < 0.01); Anxiety exhibited a negative relationship with QoL (R = −0.514, p < 0.01); Physical activity had a weak negative correlation with anxiety (R = −0.095, p < 0.01). These findings align well with theoretical expectations.
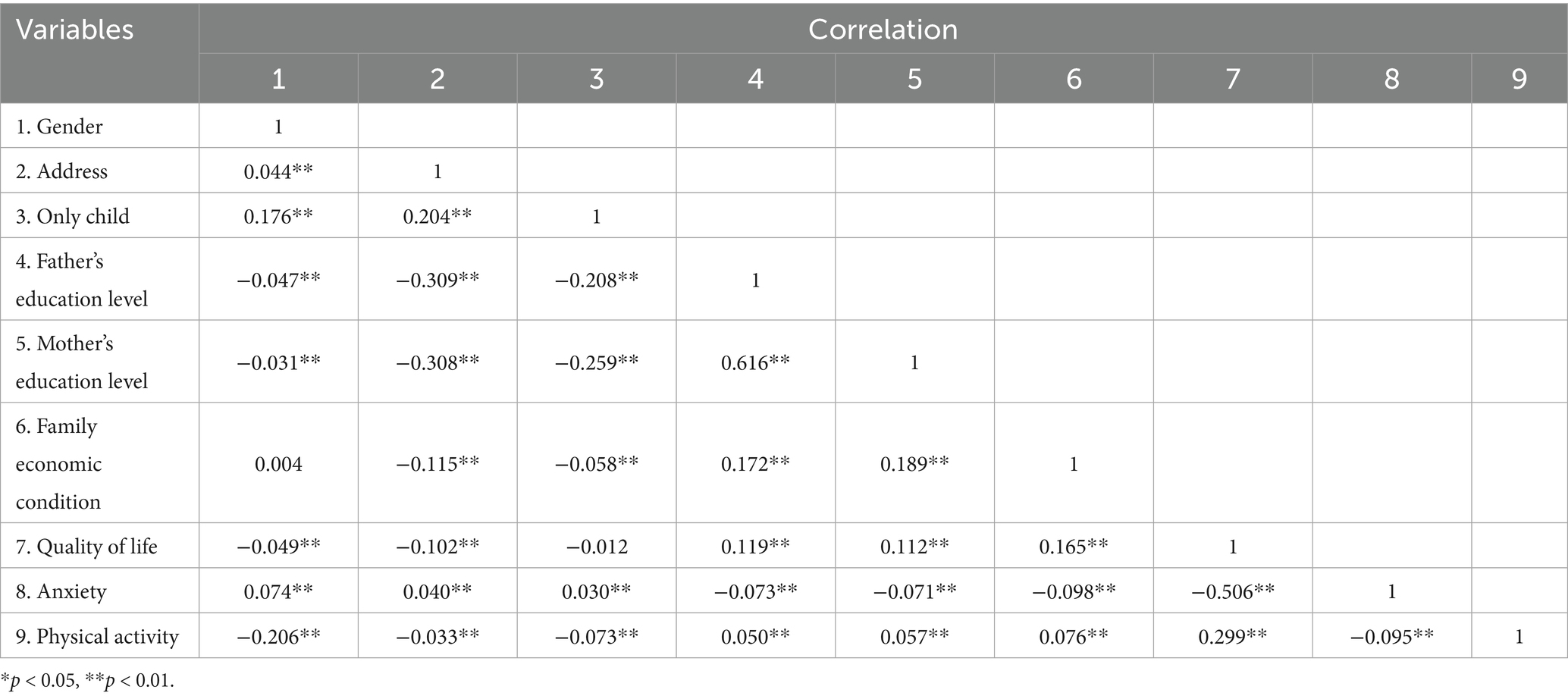
Table 2. Correlation analysis of major variables.
3.5 Hierarchical regression and mediation test
To test Hypotheses 1 (H1) and 2 (H2), Model 4 of the SPSS PROCESS macro was applied. To avoid multicollinearity between interaction terms, all independent and moderating variables were standardized. Five socio-demographic variables were included as control variables. QoL was divided into four dimensions for use in hierarchical regression and mediation analysis. The regression analysis outcomes are displayed in Table 3, while the mediation test results are summarized in Table 4.
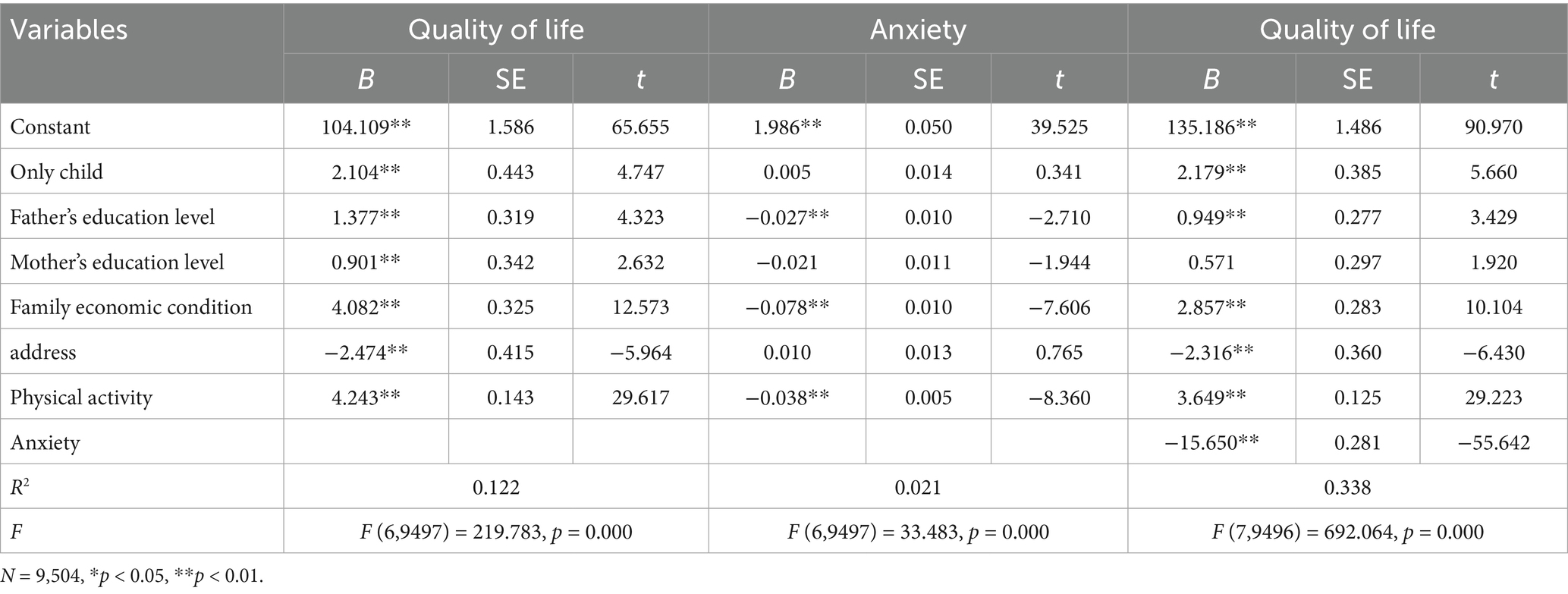
Table 3. Results of hierarchical regression analysis.
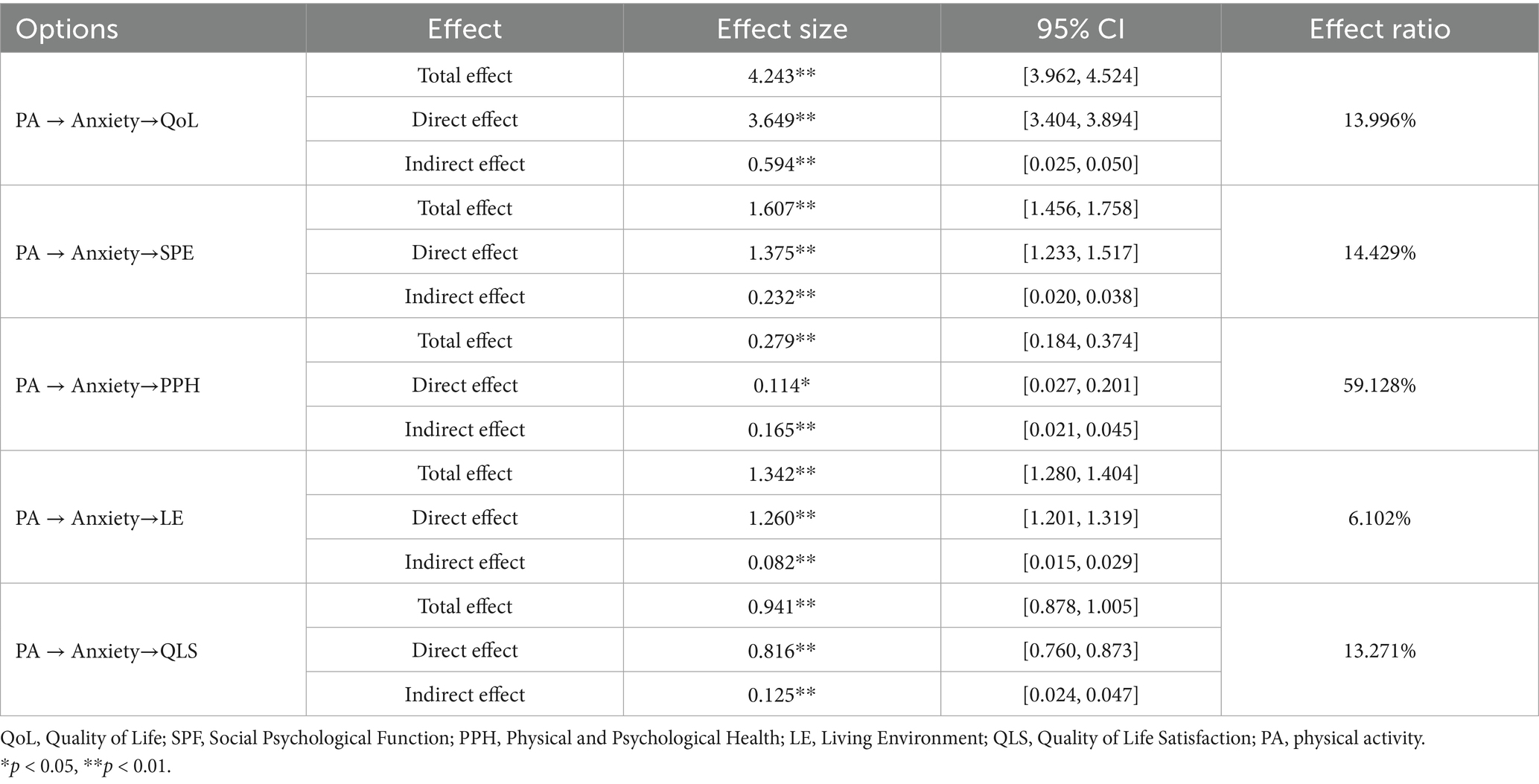
Table 4. Test of the mediating effect of anxiety.
As illustrated in Table 3, physical activity was identified as a significant positive factor for QoL (β = 4.243, p < 0.01), which aligns with H1. Moreover, physical activity significantly and negatively influenced anxiety levels (β = −0.038, p < 0.01), and anxiety also significantly and negatively affected QoL (β = −15.650, p < 0.01). These findings suggest that adolescents experience both direct improvements in QoL through physical activity and indirect benefits due to reduced anxiety. To evaluate the extent of the mediating effect, the bias-corrected percentile bootstrap method was applied (54).
As shown in Table 4, the mediating role of anxiety demonstrated an effect size of 0.594, with a 95% confidence interval spanning from (0.025, 0.050), which does not include zero—indicating a significant mediation effect. The indirect influence of physical activity on QoL mediated by anxiety constituted 13.996% of the total effect, thereby supporting H2.
3.6 Moderating effect of gender
To test the moderating role of gender, Model 59 of the SPSS PROCESS macro was applied. Five socio-demographic variables were controlled for, and all predictor variables were standardized to examine the moderated mediation model. As indicated in Table 5, gender had a significant moderating effect on the associations between physical activity and QoL (β = 0.781, p < 0.01) and between anxiety and QoL (β = 1.214, p < 0.05), lending support to Hypotheses 3 (H3) and 5 (H5). In contrast, gender did not significantly influence the relationship between physical activity and anxiety (β = 0.006, p > 0.05), thus failing to support Hypothesis 4 (H4). The results for the moderating effect of gender are shown in Table 5.
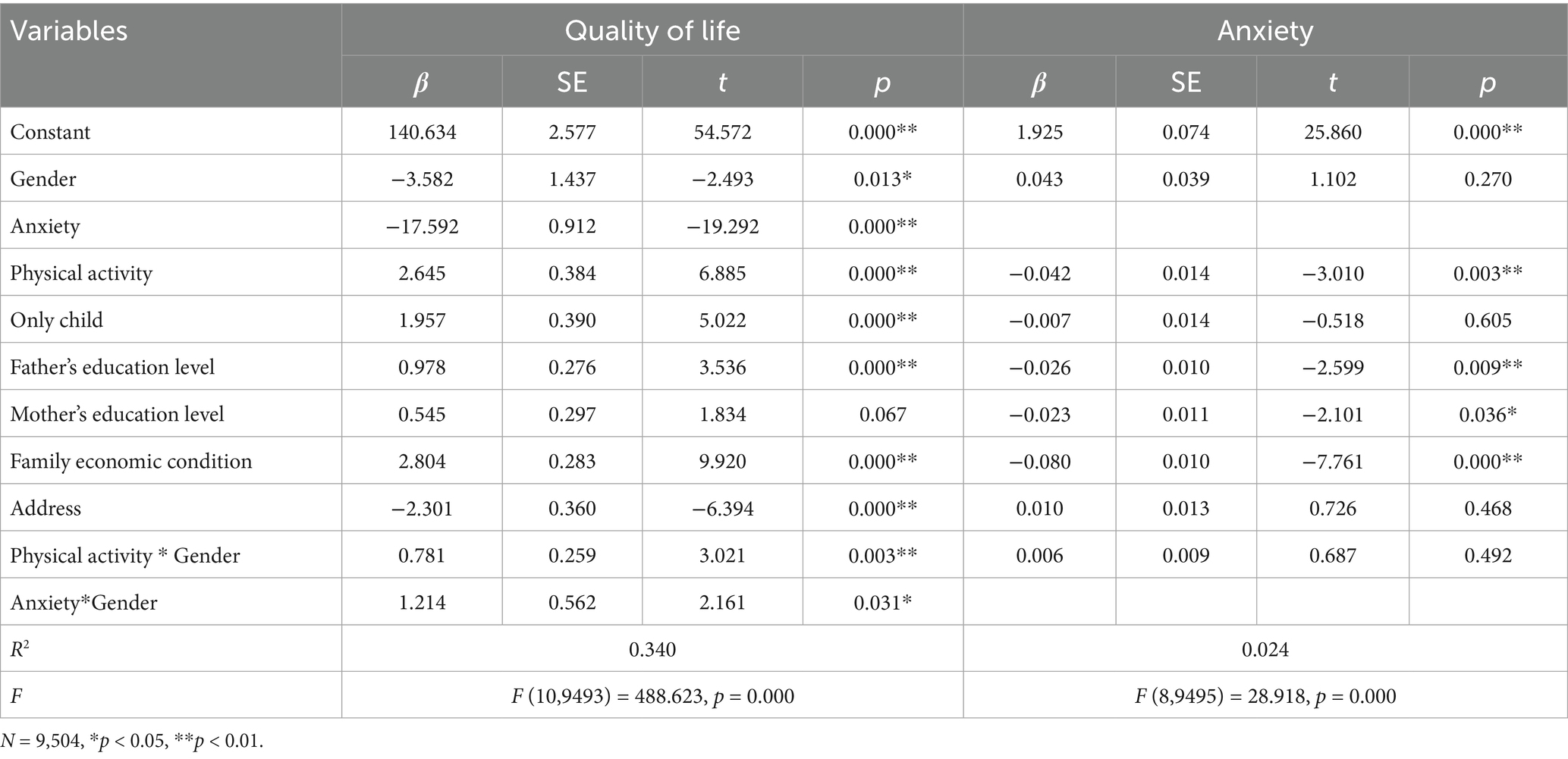
Table 5. Test on the moderating effect of gender.
In order to better examine the moderating effect of gender within the mediation model, the sample was divided into male and female groups using standardized gender scores. The relationships between physical activity and QoL, as well as between anxiety and QoL, were assessed individually for each group. As shown in Figure 3, for both male and female adolescents, higher levels of physical activity were associated with greater improvements in QoL, with the effect being more pronounced for females. Similarly, as illustrated in Figure 4, higher anxiety levels were associated with a diminished QoL in both males and females; nonetheless, the detrimental effect of anxiety on QoL was considerably more pronounced in males.
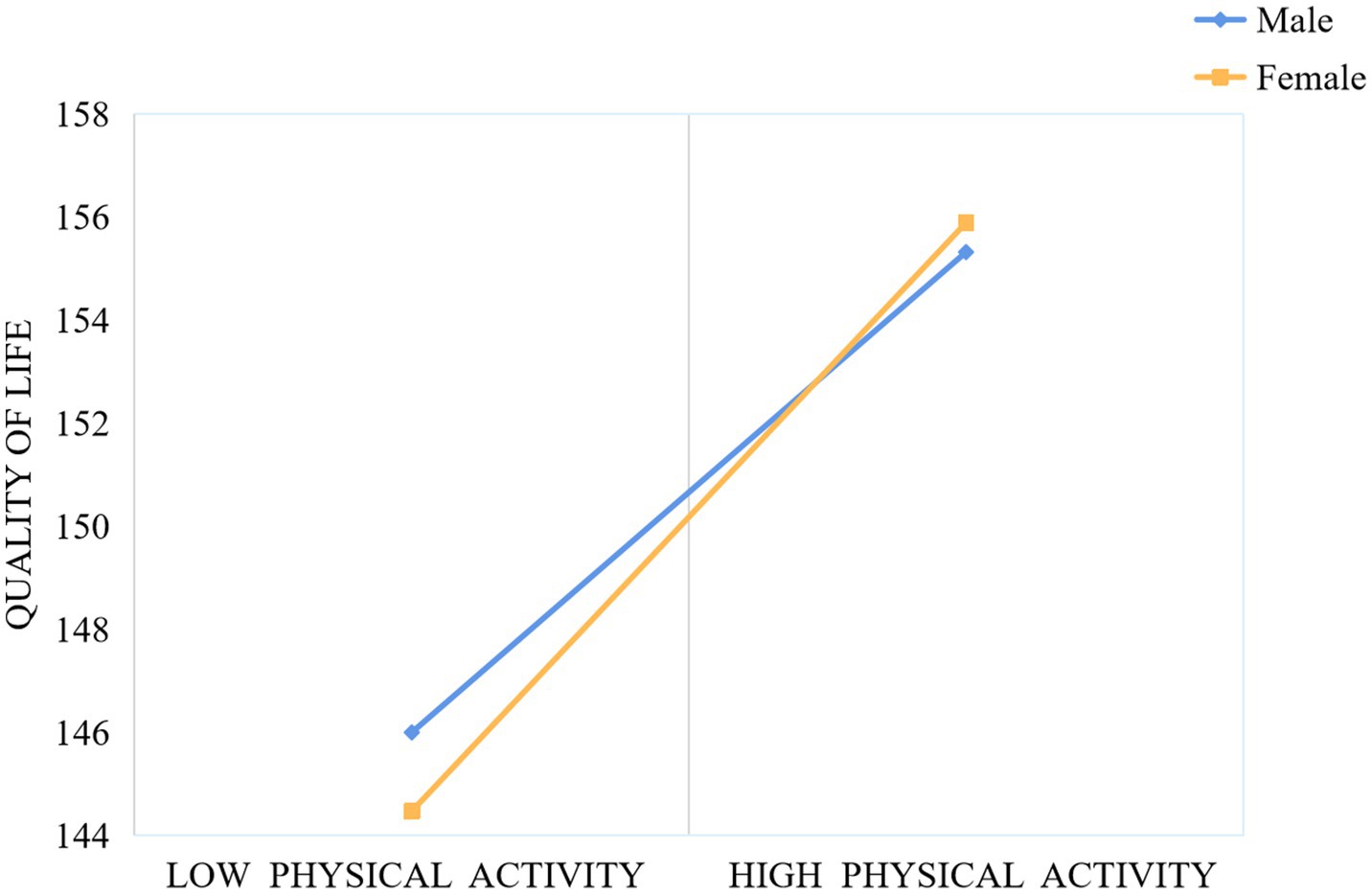
Figure 3. The moderating effect of gender on physical activity and quality of life.
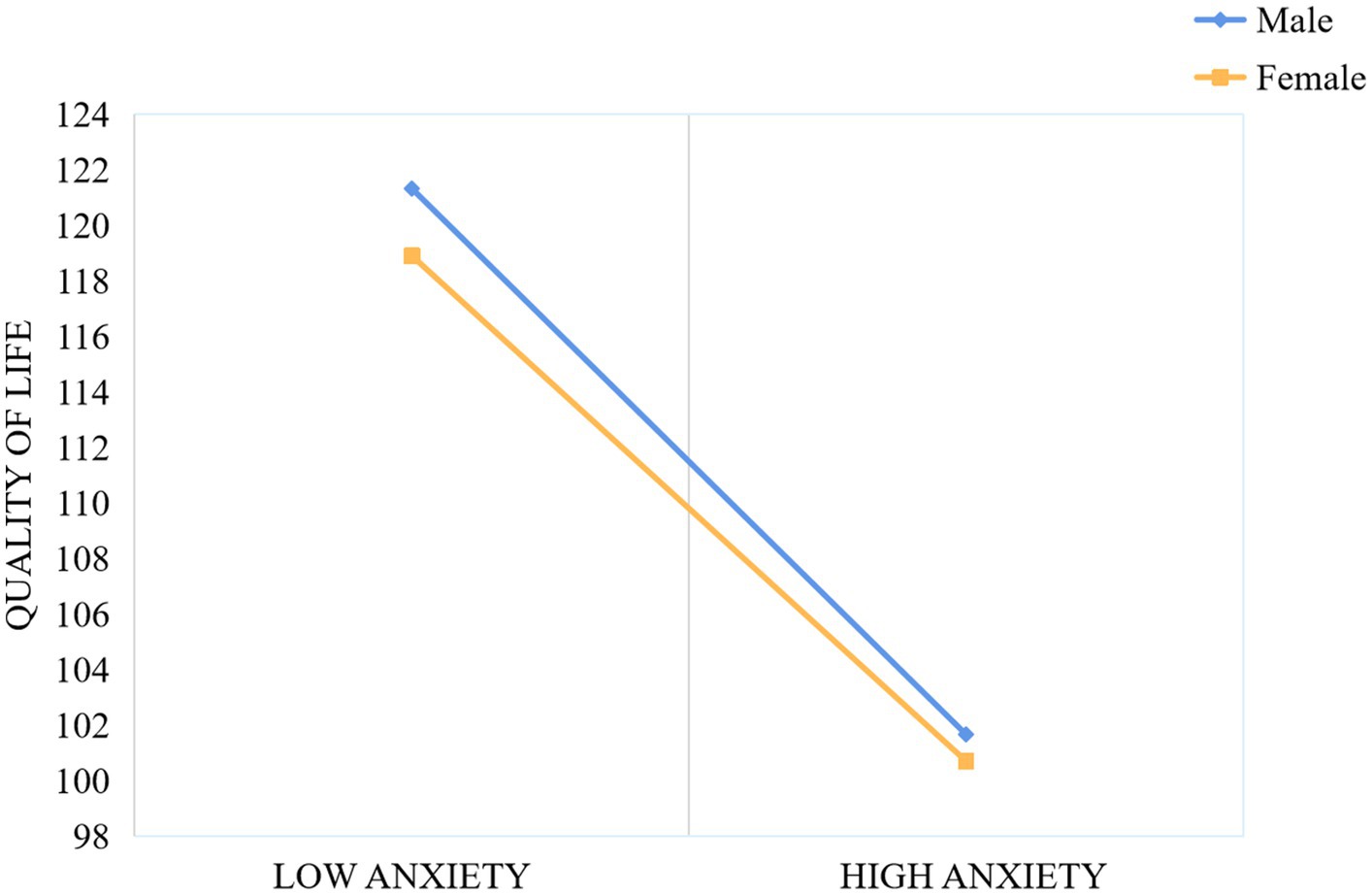
Figure 4. The moderating effect of gender on anxiety and quality of life.
3.7 Results of the moderated mediation model
As shown in Table 3, there was a significant positive association between physical activity and QoL (β = 4.243, p < 0.01), which aligns with Hypothesis 1 (H1). Moreover, anxiety played a significant mediating role in the relationship between physical activity and QoL (β = 0.594, p < 0.05), providing additional evidence for Hypothesis 2 (H2). A significant positive moderating effect of gender was found between physical activity and QoL (β = 0.781, p < 0.01), supporting Hypothesis 3 (H3). Gender also significantly moderated the relationship between anxiety and QoL (β = 1.214, p < 0.05), supporting Hypothesis 5 (H5). However, gender did not exert a statistically significant moderating effect on the relationship between physical activity and anxiety (β = 0.006, p > 0.05), thus Hypothesis 4 (H4) was not supported. The overall moderated mediation model is illustrated in Figure 5.
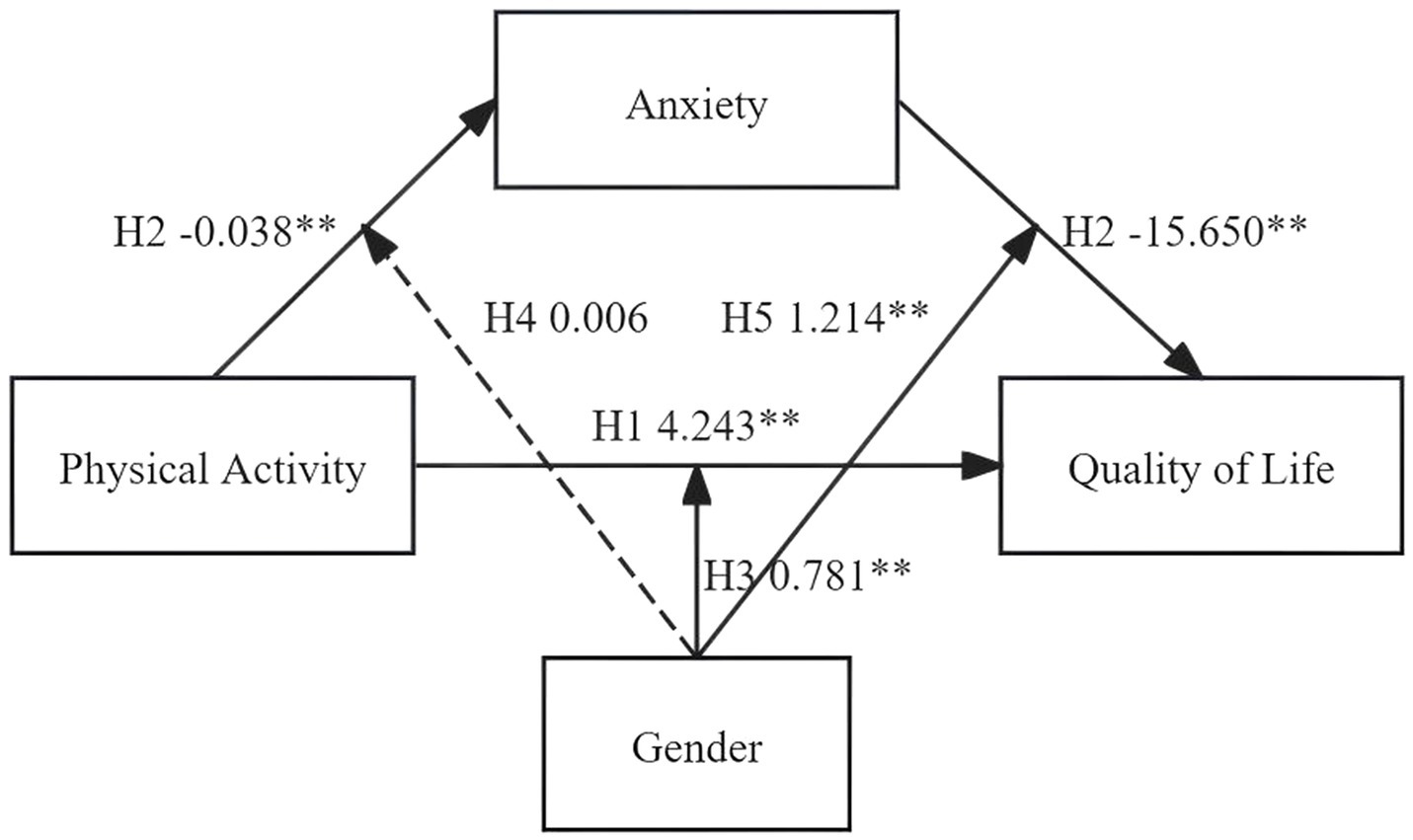
Figure 5. The results of adjusting the mediation model. *p < 0.05; **p < 0.01.
3.8 Multidimensional analysis of quality of life
In the present study, QoL was divided into four separate dimensions. Hierarchical regression analysis and mediation testing were performed using Model 4 of the SPSS PROCESS macro. The findings of the hierarchical regression analysis are provided in the Supplementary Tables 2–6, while mediation testing results are shown in Table 4. As presented in the Supplementary Tables 2–6, physical activity significantly and positively predicted four dimensions of QoL: Social Psychological Function (β = 1.607, p < 0.01), Physical and Psychological Health (β = 0.279, p < 0.01), Living Environment (β = 1.342, p < 0.01), and QoL Satisfaction (β = 0.941, p < 0.01). Furthermore, anxiety exerted a significant negative influence on these same dimensions: Social Psychological Function (β = −6.111, p < 0.01), Physical and Psychological Health (β = −4.352, p < 0.01), Living Environment (β = −2.158, p < 0.01), and QoL Satisfaction (β = −3.292, p < 0.01). As shown in Table 4, the mediation effects of anxiety across the four QoL dimensions were all statistically significant: Social Psychological Function: 14.429% (95% CI: 0.020, 0.038), Physical and Psychological Health: 59.128% (95% CI: 0.021, 0.045), Living Environment: 6.102% (95% CI: 0.015, 0.029), QoL Satisfaction: 13.271% (95% CI: 0.024, 0.047). In every instance, the confidence intervals excluded zero, which suggests a significant mediating role of anxiety. The moderating effects of gender are outlined in the Supplementary Tables 7–10: gender exerted a negative moderating influence on the relationship between anxiety and Social Psychological Function (β = −6.111, p < 0.01), gender negatively moderated the link between anxiety and Physical and Psychological Health (β = −0.503, p < 0.05), gender positively moderated the association between physical activity and Physical and Psychological Health (β = 0.729, p < 0.01), and gender positively moderated the connection between anxiety and Living Environment (β = 0.536, p < 0.01). Nevertheless, gender did not play a significant moderating role in the relationship between anxiety and QoL Satisfaction. The moderated mediation model for multidimensional QoL is depicted in Figure 6.
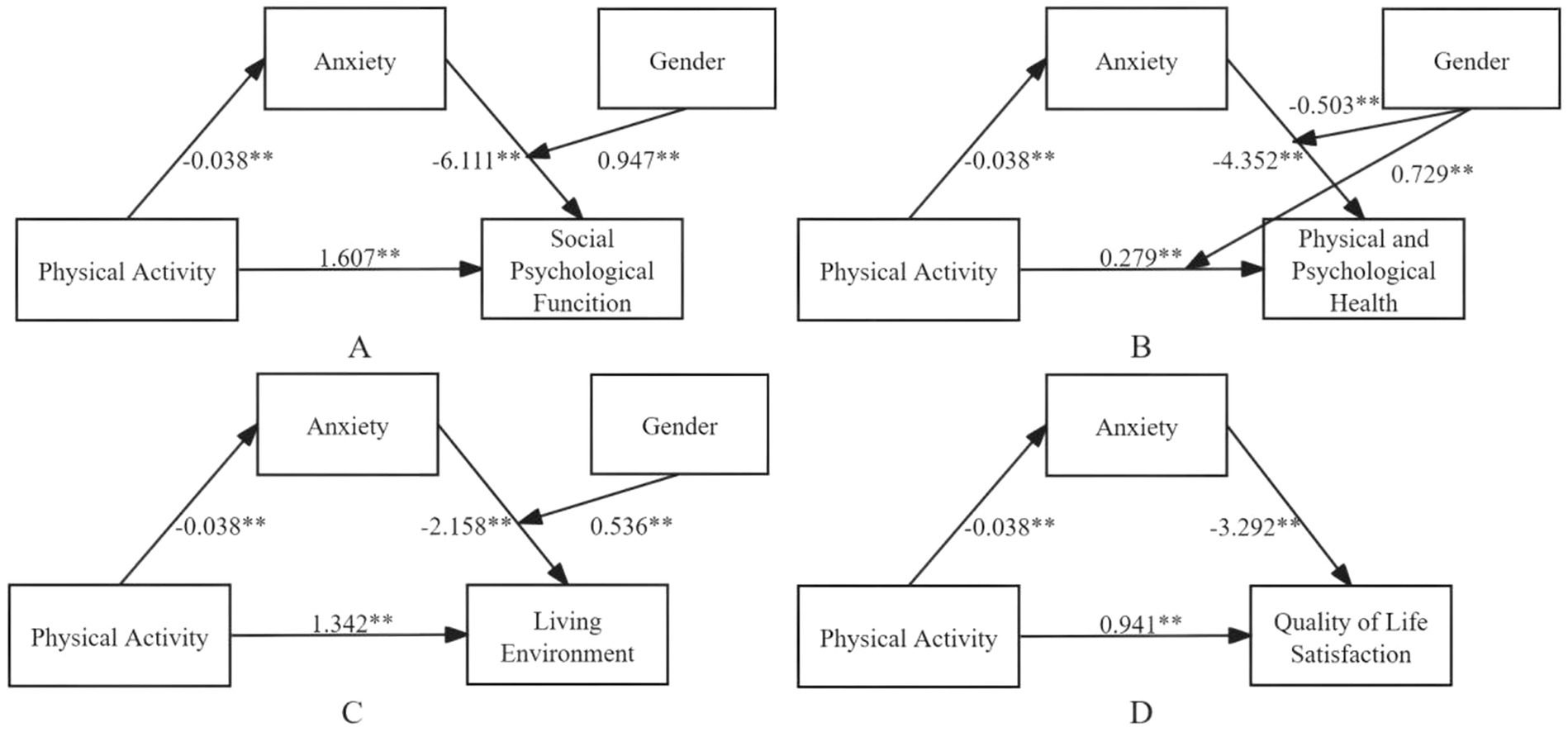
Figure 6. Results of the multi-dimensional moderating mediation model for quality of life. *p < 0.05; **p < 0.01.
4 Discussion
This study investigated the predictive effect of physical activity on QoL among adolescents and examined the potential mediating role of anxiety. The results indicated that engaging in physical activity significantly reduces anxiety, thereby positively influencing QoL. Increased physical activity levels showed a correlation with reduced anxiety and better QoL, supporting Hypotheses 1 and 2. In addition, the study demonstrated that gender significantly influenced the relationships between physical activity and QoL, as well as between anxiety and QoL, lending credence to Hypotheses 3 and 5. However, no significant moderating effect of gender was observed between physical activity and anxiety; hence, Hypothesis 4 was not supported. For both male and female adolescents, increased physical activity was associated with improved QoL, with a more pronounced effect observed among females. In contrast, anxiety had a stronger negative impact on QoL in males. A multidimensional analysis of QoL was also conducted. The results showed that gender significantly moderated the relationships between anxiety and social-psychological functioning, anxiety and physical-psychological health, anxiety and living environment, and between physical activity and physical-psychological health. However, no significant moderating effect of gender was observed on the association between anxiety and QoL Satisfaction.
4.1 Relationship between physical activity and quality of life
This study confirms the positive relationship between adolescent physical activity and QoL, consistent with existing evidence demonstrating that regular exercise enhances life satisfaction (7, 55). Importantly, these results substantiate a central tenet of Social Cognitive Theory—the mediating role of self-efficacy (56). Specifically, participation in physical activities promotes subjective well-being by strengthening adolescents’ confidence in their physical control and emotional regulation, such as through enhanced motor skills and decreased frustration-related anxiety (57). Furthermore, this finding represents a significant extension of Self-Determination Theory (58). When physical activities satisfy adolescents’ need for autonomy, sustained engagement is more likely to foster a reinforcing cycle of self-efficacy (59, 60), which can only be fully translated into improved QoL when anxiety is effectively reduced. This may explain the limited effectiveness observed in interventions that solely emphasize the general benefits of physical activity (61). Consequently, future health promotion strategies have the potential to achieve meaningful theoretical and practical advancements by prioritizing consistent participation, embedding progressive efficacy-building objectives, and integrating targeted anxiety management techniques within sport-based interventions (62), thereby maximizing QoL improvement.
4.2 Mediating role of anxiety
Modern adolescents commonly face psychological difficulties, including anxiety (63), which not only disrupt their developmental pathways (64) but also markedly degrade QoL by adversely affecting both mental and physical well-being (65) and impairing social functioning (66). Across the globe, youth are identified as a high-risk group in need of customized mental health interventions (16). Our findings indicate that engaging in physical activity can alleviate anxiety and improve QoL through a dual-mechanism process. These results further substantiate the positive association between physical activity and mental health, indicating that increased participation in exercise correlates with enhanced psychological well-being and reduced anxiety levels (62). Establishing regular physical activity patterns during adolescence not only elevates subjective well-being but also promotes mental health by mitigating symptoms of anxiety (67), stress, and depression, thereby leading to improved emotional and behavioral regulation (68, 69). At the neurobiological level, exercise supports the regulation of the hypothalamic–pituitary–adrenal (HPA) axis and stimulates neural plasticity, thus targeting the neurological origins of anxiety (31). From a psychosocial angle, involvement in team-based sports such as basketball and soccer fosters social inclusion, allowing young people to restore their self-confidence through cooperative engagement (32). The interplay between these biological and psychological processes converts anxiety reduction into observable enhancements in QoL.
It is important to recognize that the success of these mechanisms is largely shaped by local cultural values and socio-economic environments. In Shandong’s Confucian-based educational framework, rigorous academic expectations limit the time adolescents typically spend on physical activities. Nonetheless, traditional group exercises like martial arts and communal workouts can draw upon culturally significant concepts—such as collective identity—to strengthen youths’ sense of personal capability (70). Economic inequality further widens the gap due to unequal distribution of resources; families with limited income may struggle with anxiety management owing to scarce access to public recreational facilities and insufficient awareness of the benefits of physical activity (71).
Hence, embedding physical activity as a central approach for anxiety prevention should start at the neurophysiological level by introducing high-intensity interval training (HIIT) in middle schools; research indicates that just one 20-min session can improve HPA axis function (72). Secondly, from a cultural integration perspective, brief, school-based physical activities—such as five-minute seated movement breaks—should be embedded into the daily schedule, while promoting collectivist principles through team-oriented reward systems (32, 73). Finally, to promote equity across different socio-economic levels, low-cost and community-centered sports initiatives must be expanded for underserved groups, including equipment-sharing programs, and formal channels for school team involvement should be created to remove participation obstacles.
4.3 Moderating role of gender
Theoretical frameworks suggest that gender differences in physical activity are shaped by biological, psychological, cognitive, and socio-developmental factors (74). Gender significantly influences both motivation and outcomes in physical activity, which may relate to psychological needs, participation motives, and satisfaction levels (75, 76). Due to inherent physiological differences, males typically exhibit greater spontaneity, engagement, and competence in physical activity (76, 77). However, with increasing participation, females report greater emotional, social, and self-perceptual satisfaction from physical activity (78). Long-term health benefits for females include higher activity levels, lower BMI, and reduced obesity risk (79).
Meta-analyses show that females experience greater QoL improvements from physical activity, especially in the domains of physical functioning and social roles (80), indicating that its indirect effects are more pronounced among females (81, 82). Simultaneously, females demonstrate a greater capacity to utilize social interactions in team sports to alleviate anxiety. Evidence also suggests that females experience lower levels of anxiety than males (83). Males exhibit higher levels of anxiety and depression, both of which strongly affect their QoL (84). Anxiety-related declines in QoL are common among young males (85), and studies among college students have found that males have lower psychological and social QoL when anxiety is clinically significant. Research in China has also noted that males are more susceptible to psychological stressors, leading to reduced QoL (86). These findings align with the current study: physical activity improves QoL more significantly for females, whereas anxiety more severely compromises QoL for males.
This natural physiological tendency is further influenced by sociocultural norms. In particular, dominant societal expectations often push men to display “masculinity” through competitive achievement, which may restrict emotional openness and cause unaddressed anxiety to manifest as physical symptoms, thus impairing QoL (87). On the other hand, the sense of connection that women gain from collaborative activities can act as a buffer against stressors tied to academic pressure and appearance-related issues (88); however, unequal access to resources hampers the full realization of these benefits (89). These outcomes correspond with the findings of the present research, which suggest that physical activity has a more favorable effect on women’s QoL, while men are more likely to suffer from anxiety-related negative impacts. Based on these gender-specific mechanisms (90), healthcare practices should consider targeted interventions—embedding emotional regulation techniques into male-oriented competitive sports (91) and providing affordable, group-focused programs designed for women (92).
4.4 Multidimensional analysis of quality of life
Earlier research has demonstrated that engaging in physical activity may lower anxiety levels, leading to enhancements in various dimensions of QoL—such as physical-psychological health, social relationships, and environmental adaptation—among adolescents (93, 94). Anxiety serves as a significant mediator, confirming its central role in the physical activity—QoL relationship (95). Our results align with this notion, indicating that physical activity enhances four dimensions of QoL—social-psychological functioning, physical-psychological health, living environment, and satisfaction with QoL—by mediating the effect through anxiety. Notably, gender did not play a significant moderating role in the association between anxiety and QoL satisfaction. In contrast, gender exhibited a negative moderating effect on the relationship between anxiety and physical-psychological health. Among the various moderated mediation effects, only the dimension of physical-psychological health exhibited a significant moderating effect of gender. This may be attributed to the interaction between biological responses and social role expectations. Some studies suggest that QoL Satisfaction is influenced more by individual subjectivity and less by gender (96). Anxiety more strongly affects physical-psychological health, social functioning, and environmental dimensions (83), with its impact on female QoL being especially pronounced in health-related outcomes (97). Other studies support our finding that gender differences primarily appear in the effects of physical activity on physical and psychological health, while effects on social and environmental dimensions are not significantly moderated by gender (98, 99).
However, this emphasizes the importance of future studies focusing on uncovering the mechanisms involved in this particular dimension. As a result, upcoming research should incorporate more detailed variables, such as specific neurobiological markers (100), objective indicators of physiological stress responses (101), and in-depth analyses of sociocultural norms (102). Moreover, utilizing advanced research methodologies—including longitudinal study designs (103), real-time physiological measurements (104)—can greatly improve the rigor of such investigations. These methodological improvements will facilitate a more accurate understanding of how biological and sociocultural elements interact dynamically through gender-specific pathways in the realm of physical-psychological health. This area of research is anticipated to shed light on the underlying causes of existing disparities and guide the creation of focused, evidence-driven intervention strategies. In the long run, thorough investigation in this field may lead to the identification of more gender-responsive methods for promoting equitable health outcomes.
4.5 Limitations
This research examined the mediating effect of anxiety on the relationship between physical activity and QoL among adolescents and assessed the moderating influence of gender. A comprehensive multidimensional analysis of QoL was also conducted. The large and diverse sample provides broad representativeness, offering a realistic reflection of adolescents’ experiences. The findings offer new insights into adolescent health promotion mechanisms and provide empirical support for differentiated intervention strategies.
Although this study has notable strengths, several limitations should be considered in future research. First, the cross-sectional design identifies associations but does not support causal conclusions. Therefore, the proposed pathway—"physical activity → reduced anxiety → improved quality of life”—remains speculative. While statistical methods were used to examine mediation and moderation, unmeasured variables or alternative models may also explain the results. The actual mechanisms may be more complex than identified. Second, anxiety was measured only with the SCL-90 anxiety subscale, which captures emotional distress but misses key physical and behavioral symptoms—such as somatic discomfort and avoidance—that are central to anxiety disorders. This limits understanding of how anxiety interacts with physical activity and QoL. Physical activity was assessed through self-report (PAQ-A), which is prone to recall errors and social desirability bias, possibly leading to overestimation. In addition, data collected at a single time point cannot reflect dynamic changes or long-term trends. Third, although the sample was large and representative within Shandong Province, findings may not generalize to other regions or countries due to differences in culture, economy, and education. Studies in diverse contexts are needed to improve external validity. Also, since participants were aged 12–18, results may not apply to younger children or young adults. Lastly, while gender was examined as a moderator, other factors such as being an only child, parental education, and family socioeconomic status were included only as controls. Their potential moderating effects were not analyzed. Future studies should explore these variables in depth to better understand contextual influences on the studied relationships.
5 Conclusion
In summary, the following conclusions can be drawn: Adolescent physical activity significantly enhances QoL. Active participation in physical exercise is an effective means to promote overall adolescent well-being. Engaging in physical activity enhances QoL both directly and indirectly through the reduction of anxiety. Increased physical activity correlates with decreased anxiety, which subsequently leads to an improvement in QoL. The influence of physical activity and anxiety on QoL varies across genders, as gender acts as a moderating factor in this relationship. Female adolescents experience more substantial improvements in happiness and QoL through physical activity, while male adolescents are more vulnerable to anxiety-related declines in QoL. The impact of physical activity on different QoL dimensions is mediated by anxiety and moderated by gender, indicating the presence of both universal and gender-specific mechanisms. These findings provide a theoretical foundation for using physical activity as an intervention to improve adolescent mental health and QoL and highlight the importance of gender-sensitive strategies in policy and practice.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://www.ncmi.cn/phda/dataDetails.do?id=CSTR:17970.11.A0031.202107.209.V1.0.
Ethics statement
The studies involving humans were approved by Ethics Committee of Shandong University (20180517). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
SM: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. YG: Funding acquisition, Supervision, Writing – review & editing. LZ: Conceptualization, Data curation, Writing – original draft. WS: Data curation, Methodology, Writing – original draft. YY: Conceptualization, Methodology, Writing – original draft. YH: Data curation, Methodology, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the National Social Science Foundation of China (grant number: 21BTY054).
Acknowledgments
We appreciate the contributions of all staff who helped collect the data. Thanks to the support of the National Social Science Fund of China and Shandong University.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1625066/full#supplementary-material
References
1. Kuyken, W, Orley, J, Power, M, Herrman, H, Schofield, H, Murphy, B, et al. The world-health-organization quality-of-life assessment (WHOQOL) - position paper from the world-health-organization. Soc Sci Med. (1995) 41:1403–9. doi: 10.1016/0277-9536(95)00112-k
2. Liu, WJ, Zhou, L, Wang, XQ, Yang, BX, Wang, Y, and Jiang, JF. Mediating role of resilience in relationship between negative life events and depression among Chinese adolescents. Arch Psychiatr Nurs. (2019) 33:116–22. doi: 10.1016/j.apnu.2019.10.004
3. Haraldstad, K, Wahl, A, Andenaes, R, Andersen, JR, Andersen, MH, Beisland, E, et al. A systematic review of quality of life research in medicine and health sciences. Qual Life Res. (2019) 28:2641–50. doi: 10.1007/s11136-019-02214-9
4. WHO, (2025) Adolescent health. Available online at: https://www.who.int/health-topics/adolescent-health [Accessed June 25, 2025]
5. Babapour, A-R, Gahassab-Mozaffari, N, and Fathnezhad-Kazemi, A. Nurses' job stress and its impact on quality of life and caring behaviors: a cross-sectional study. BMC Nurs. (2022) 21:75. doi: 10.1186/s12912-022-00852-y
6. Viner, R, Russell, S, Saulle, R, Croker, H, Stansfield, C, Packer, J, et al. School closures during social lockdown and mental health, health behaviors, and well-being among children and adolescents during the first COVID-19 wave: a systematic review. JAMA Pediatr. (2022) 176:400–9. doi: 10.1001/jamapediatrics.2021.5840
7. Djerioui, M, Abderrahim, L, and Lebchiri, A. The impact of practicing sports and physical activities on life quality level among a sample of master's students after the corona pandemic. Phys Educ Stud. (2024) 28:43–51. doi: 10.15561/20755279.2024.0105
8. Dufner, M, Gebauer, JE, Sedikides, C, and Denissen, JJA. Self-enhancement and psychological adjustment: a meta-analytic review. Personal Soc Psychol Rev. (2019) 23:48–72. doi: 10.1177/1088868318756467
9. Wu, HL, Liu, PL, and Meng, H. Analysis of the reliability and validity of the quality of life scale for children and adolescents and formulation of the national norm. Chin J Sch Health. (2006) 7:18–21.
10. Hao, Y, Sun, X, Duan, W, Fong, DYT, and Jin, X. A moving target: exploring if, when, how, and why promoting quality of life counts among children and adolescents during the COVID-19 pandemic. Front Public Health. (2023) 11:1339945. doi: 10.3389/fpubh.2023.1339945
11. Ravens-Sieberer, U, Kaman, A, Erhart, M, Devine, J, Schlack, R, and Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur Child Adolesc Psychiatry. (2022) 31:879–89. doi: 10.1007/s00787-021-01726-5
12. Duan, W, Kong, Y, Bu, H, Guan, Q, Chen, Z, Luo, Q, et al. The online strength-informed acceptance and commitment therapy among COVID-19-affected adolescents. Res Soc Work Pract. (2022) 32:465–74. doi: 10.1177/10497315211067270
13. Silva, A, Monteiro, D, and Sobreiro, P. Effects of sports participation and the perceived value of elite sport on subjective well-being. Sport Soc. (2020) 23:1202–16. doi: 10.1080/17430437.2019.1613376
14. Helseth, S, and Misvær, N. Adolescents' perceptions of quality of life: what it is and what matters. J Clin Nurs. (2010) 19:1454–61. doi: 10.1111/j.1365-2702.2009.03069.x
15. Wu, XY, Han, LH, Zhang, JH, Luo, S, Hu, JW, and Sun, K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLoS One. (2017) 12:e0187668. doi: 10.1371/journal.pone.0187668
16. Ammar, A, Mueller, P, Trabelsi, K, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Psychological consequences of COVID-19 home confinement: the ECLB-COVID19 multicenter study. PLoS One. (2020) 15:e0240204. doi: 10.1371/journal.pone.0240204
17. Ammar, A, Trabelsi, K, Brach, M, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: insight from the ECLB-COVID19 multicenter study. Biol Sport. (2021) 38:9–21. doi: 10.5114/biolsport.2020.96857
18. Brooks, SK, Webster, RK, Smith, LE, Woodland, L, Wessely, S, Greenberg, N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
19. Jackson, SB, Stevenson, KT, Larson, LR, Peterson, MN, and Seekamp, E. Outdoor activity participation improves adolescents' mental health and well-being during the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:2506. doi: 10.3390/ijerph18052506
20. Liu, R, Menhas, R, and Saqib, ZA. Does physical activity influence health behavior, mental health, and psychological resilience under the moderating role of quality of life? Front Psychol. (2024) 15:1349880. doi: 10.3389/fpsyg.2024.1349880
21. Shek, DTL. COVID-19 and quality of life: twelve reflections. Appl Res Qual Life. (2021) 16:1–11. doi: 10.1007/s11482-020-09898-z
22. Hargreaves, D, Mates, E, Menon, P, Alderman, H, Devakumar, D, Fawzi, W, et al. Strategies and interventions for healthy adolescent growth, nutrition, and development. Lancet. (2022) 399:198–210. doi: 10.1016/S0140-6736(21)01593-2
23. GBD results. (2025) Institute of health metrics and evaluation. https://vizhub.healthdata.org/gbd-results [Accessed June 25, 2025]
24. WHO, (2025) Mental health of adolescents. https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health [Accessed June 25, 2025]
25. Zhang, Y, and Ma, ZF. Impact of the COVID-19 pandemic on mental health and quality of life among local residents in Liaoning province, China: a cross-sectional study. Int J Environ Res Public Health. (2020) 17:2381. doi: 10.3390/ijerph17072381
26. Aqeel, M, Rehna, T, Shuja, KH, and Abbas, J. Comparison of students' mental wellbeing, anxiety, depression, and quality of life during COVID-19's full and partial (smart) lockdowns: a follow-up study at a 5-month interval. Front Psych. (2022) 13:835585. doi: 10.3389/fpsyt.2022.835585
27. Han, G-S, and Park, J-A. The relationship between parental academic achievement pressure, physical activity, self-esteem, and body image among south Korean adolescents. Adolescents. (2024) 4:484–92. doi: 10.3390/adolescents4040034
28. Bai, W, Zhao, Y-J, Cai, H, Sha, S, Zhang, Q, Lei, S-M, et al. Network analysis of depression, anxiety, insomnia and quality of life among Macau residents during the COVID-19 pandemic. J Affect Disord. (2022) 311:181–8. doi: 10.1016/j.jad.2022.05.061
29. Mahindru, A, Patil, P, and Agrawal, V. Role of physical activity on mental health and well-being: a review. Cureus. (2023) 15:e33475. doi: 10.7759/cureus.33475
30. Andermo, S, Hallgren, M, Nguyen, T-T-D, Jonsson, S, Petersen, S, Friberg, M, et al. School-related physical activity interventions and mental health among children: a systematic review and meta-analysis. Sports Med Open. (2020) 6:25. doi: 10.1186/s40798-020-00254-x
31. Stonerock, GL, Hoffman, BM, Smith, PJ, and Blumenthal, JA. Exercise as treatment for anxiety: systematic review and analysis. Ann Behav Med. (2015) 49:542–56. doi: 10.1007/s12160-014-9685-9
32. Solmaz, S, İnan, M, and Şahin, MY. The moderating effects of physical activity on social anxiety and sleep disturbance: managing gaming disorder in young e-sports players. Front Public Health. (2025) 13:44. doi: 10.3389/fpubh.2025.1544044
34. Deci, EL, and Ryan, RM. Intrinsic motivation and self-determination in human behavior. New York: Plenum (1985).
35. Ferriz, R, Gonzalez-Cutre, D, and Balaguer-Gimenez, J. Agents of the educational community, novelty satisfaction, and physical activity. Cult Cienc Deporte. (2020) 15:519–28. doi: 10.12800/CCD.V15I46.1602
36. Hamer, M, and Steptoe, A. Cortisol responses to mental stress and incident hypertension in healthy men and women. J Clin Endocrinol Metab. (2012) 97:E29–34. doi: 10.1210/jc.2011-2132
37. Hill, EE, Zack, E, Battaglini, C, Viru, M, Viru, A, and Hackney, AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Investig. (2008) 31:587–91. doi: 10.1007/BF03345606
38. Chrousos, GP. Stress and disorders of the stress system. Nat Rev Endocrinol. (2009) 5:374–81. doi: 10.1038/nrendo.2009.106
39. Horesh, D, Kapel Lev-Ari, R, and Hasson-Ohayon, I. Risk factors for psychological distress during the COVID-19 pandemic in Israel: loneliness, age, gender, and health status play an important role. Br J Health Psychol. (2020) 25:925–33. doi: 10.1111/bjhp.12455
40. Solomou, I, and Constantinidou, F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: age and sex matter. Int J Environ Res Public Health. (2020) 17:4924. doi: 10.3390/ijerph17144924
41. Eagly, AH, and Wood, W. The nature-nurture debates: 25 years of challenges in understanding the psychology of gender. Perspect Psychol Sci. (2013) 8:340–57. doi: 10.1177/1745691613484767
42. Hyde, JS. Gender similarities and differences. Annu Rev Psychol. (2014) 65:373–98. doi: 10.1146/annurev-psych-010213-115057
43. Nolen-Hoeksema, S, and Girgus, JS. The emergence of gender differences in depression during adolescence. Psychol Bull. (1994) 115:424–43. doi: 10.1037/0033-2909.115.3.424
44. Rose, AJ, and Rudolph, KD. A review of sex differences in peer relationship processes: potential trade-offs for the emotional and behavioral development of girls and boys. Psychol Bull. (2006) 132:98–131. doi: 10.1037/0033-2909.132.1.98
45. Rodríguez-Naranjo, C, and Caño, A. Daily stress and coping styles in adolescent hopelessness depression: moderating effects of gender. Pers Individ Differ. (2016) 97:109–14. doi: 10.1016/j.paid.2016.03.027
46. Li, X, Wang, Y, Li, XT, Li, DF, Sun, C, Xie, MH, et al. Revision and reliability and validity study of the Chinese version of the adolescent physical activity questionnaire (PAQ-A). J Beijing Sport Univ. (2015) 38:63–7. doi: 10.19582/j.cnki.11-3785/g8.2015.05.012
47. Bujang, MA, Omar, ED, and Baharum, NA. A review on sample size determination for Cronbach's alpha test: a simple guide for researchers. Malays J Med Sci. (2018) 25:85–99. doi: 10.21315/mjms2018.25.6.9
48. Ayabe, N, Okajima, I, Yamadera, W, Tachimori, H, Yamashita, H, Uchimura, N, et al. Development, reliability, and validity of the quality of life scale for insomnia: a health-related quality of life instrument for insomnia. Front Psych. (2025) 16:1538148. doi: 10.3389/fpsyt.2025.1538148
49. Derogatis, LR, and Cleary, PA. Confirmation of the dimensional structure of the scl-90: a study in construct validation. J Clin Psychol. (1977) 33:981–9. doi: 10.1002/1097-4679(197710)33:4<981::AID-JCLP2270330412>3.0.CO;2-0
50. Yang, Z, and Killian, MO. A systematic review of anxiety measurement scales in pediatric organ transplantation patients. Prog Transplant. (2025) 35:22–40. doi: 10.1177/15269248241305018
51. Faber, J, and Fonseca, LM. How sample size influences research outcomes. Dent Press J Orthod. (2014) 19:27–9. doi: 10.1590/2176-9451.19.4.027-029.ebo
52. Podsakoff, PM, MacKenzie, SB, Lee, J-Y, and Podsakoff, NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. (2003) 88:879–903. doi: 10.1037/0021-9010.88.5.879
53. George, D, and Mallery, P. IBM SPSS statistics 25 step by step a simple guide and reference a simple guide and reference. New York: Routledge (2019).
54. He, MX, Li, C, and Zhao, M. Simulation comparison of interval estimation methods for non-normal population means. Sci Technol Inform. (2009) 16:971–2.
55. Miao, XL, and Bian, YJ. Epidemic prevention, social capital, physical exercise and physical and mental health. J Shanghai Univ Sport. (2020) 44:1–12. doi: 10.16099/j.sus.2020.12.001
56. Young, MD, Plotnikoff, RC, Collins, CE, Callister, R, and Morgan, PJ. Social cognitive theory and physical activity: a systematic review and meta-analysis. Obes Rev. (2014) 15:983–95. doi: 10.1111/obr.12225
57. Marquez, DX, Aguiñaga, S, Vásquez, PM, Conroy, DE, Erickson, KI, Hillman, C, et al. A systematic review of physical activity and quality of life and well-being. Transl Behav Med. (2020) 10:1098–109. doi: 10.1093/tbm/ibz198
58. Standage, M, Duda, JL, and Ntoumanis, N. A model of contextual motivation in physical education: using constructs from self-determination and achievement goal theories to predict physical activity intentions. J Educ Psychol. (2003) 95:97–110. doi: 10.1037/0022-0663.95.1.97
59. Ana-Maria, V. Satisfaction of participants in physical activity programs as an indicator of quality of life. Procedia Soc Behav Sci. (2015) 180:1434–8. doi: 10.1016/j.sbspro.2015.02.289
60. Venter, Dewald, and Kruger, Stefan. (2025) "Soldiers of paint": relationship between leisure adventure combat sport and quality of life. Available online at: https://webofscience.clarivate.cn/wos/alldb/full-record/WOS:000427229000012 [Accessed April 23, 2025]
61. Moeijes, J, Van Busschbach, JT, Bosscher, RJ, and Twisk, JWR. Sports participation and health-related quality of life: a longitudinal observational study in children. Qual Life Res. (2019) 28:2453–69. doi: 10.1007/s11136-019-02219-4
62. White, RL, Babic, MJ, Parker, PD, Lubans, DR, Astell-Burt, T, and Lonsdale, C. Domain-specific physical activity and mental health: a meta-analysis. Am J Prev Med. (2017) 52:653–66. doi: 10.1016/j.amepre.2016.12.008
63. Cao, X, Zhang, Q, and Liu, X. Cross-lagged relationship between physical activity time, openness and depression symptoms among adolescents: evidence from China. Int J Ment Health Promot. (2023) 25:1009–18. doi: 10.32604/ijmhp.2023.029365
64. George, A, and Moolman, R. Resilience and suicide ideation: coping mediator-moderator effects among adolescent learners. J Psychol Afr. (2017) 27:494–502. doi: 10.1080/14330237.2017.1375214
65. Schultchen, D, Reichenberger, J, Mittl, T, Weh, TRM, Smyth, JM, Blechert, J, et al. Bidirectional relationship of stress and affect with physical activity and healthy eating. Br J Health Psychol. (2019) 24:315–33. doi: 10.1111/bjhp.12355
66. Momen, NC, Plana-Ripoll, O, Agerbo, E, Benros, ME, Borglum, AD, Christensen, MK, et al. Association between mental disorders and subsequent medical conditions. N Engl J Med. (2020) 382:1721–31. doi: 10.1056/NEJMoa1915784
67. Rodriguez-Ayllon, M, Cadenas-Sanchez, C, Estevez-Lopez, F, Munoz, NE, Mora-Gonzalez, J, Migueles, JH, et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: a systematic review and meta-analysis. Sports Med. (2019) 49:1383–410. doi: 10.1007/s40279-019-01099-5
68. Brown, HE, Pearson, N, Braithwaite, RE, Brown, WJ, and Biddle, SJH. Physical activity interventions and depression in children and adolescents: a systematic review and meta-analysis. Sports Med. (2013) 43:195–206. doi: 10.1007/s40279-012-0015-8
69. Teuber, M, Leyhr, D, and Sudeck, G. Physical activity improves stress load, recovery, and academic performance-related parameters among university students: a longitudinal study on daily level. BMC Public Health. (2024) 24:598. doi: 10.1186/s12889-024-18082-z
70. Du, H, Li, X, Lin, D, and Tam, CC. Collectivistic orientation, acculturative stress, cultural self-efficacy, and depression: a longitudinal study among Chinese internal migrants. Community Ment Health J. (2015) 51:239–48. doi: 10.1007/s10597-014-9785-9
71. Luo, D, Ma, N, Liu, Y, Yan, X, Ma, J, Song, Y, et al. Long-term trends and urban-rural disparities in the physical growth of children and adolescents in China: an analysis of five national school surveys over three decades. Lancet Child Adolesc Health. (2023) 7:762–72. doi: 10.1016/S2352-4642(23)00175-X
72. Costigan, SA, Eather, N, Plotnikoff, RC, Hillman, CH, and Lubans, DR. High-intensity interval training for cognitive and mental health in adolescents. Med Sci Sports Exerc. (2016) 48:1985–93. doi: 10.1249/MSS.0000000000000993
73. Ho, FKW, Louie, LHT, Chow, CB, Wong, WHS, and Ip, P. Physical activity improves mental health through resilience in Hong Kong Chinese adolescents. BMC Pediatr. (2015) 15:48. doi: 10.1186/s12887-015-0365-0
74. Cooper, AR, Goodman, A, Page, AS, Sherar, LB, Esliger, DW, van Sluijs, EMF, et al. Objectively measured physical activity and sedentary time in youth: the international children's accelerometry database (ICAD). Int J Behav Nutr Phys Act. (2015) 12:113. doi: 10.1186/s12966-015-0274-5
75. Pfister, G. Women in sport – gender relations and future perspectives1. Sport Soc. (2010) 13:234–48. doi: 10.1080/17430430903522954
76. Crocker, PRE, and Augaitis, L. Commitment in age class adult triathletes: examining gender differences in the sport commitment model. Int J Sport Psychol. (2010) 41:177–94.
77. Steene-Johannessen, J, Hansen, BH, Dalene, KE, Kolle, E, Northstone, K, Møller, NC, et al. Variations in accelerometry measured physical activity and sedentary time across Europe – harmonized analyses of 47,497 children and adolescents. Int J Behav Nutr Phys Act. (2020) 17:38. doi: 10.1186/s12966-020-00930-x
78. Chen, JA, Yin, RB, Liu, JH, and Chen, PY. A correlation study on the participation factors of leisure sports among middle school students of different genders. J Chengdu Sport Univ. (2017) 43:113–9. doi: 10.15942/j.jcsu.2017.02.020
79. Kaestner, R, and Xu, X. Title IX, girls' sports participation, and adult female physical activity and weight. Eval Rev. (2010) 34:52–78. doi: 10.1177/0193841X09353539
80. Karmali, KN, Davies, P, Taylor, F, Beswick, A, Martin, N, and Ebrahim, S. Promoting patient uptake and adherence in cardiac rehabilitation. Cochrane Database Syst Rev. (2014) 6:CD007131. doi: 10.1002/14651858.CD007131.pub3
81. Stracciolini, A, Amar-Dolan, L, Howell, DR, Alex, T, Berkner, P, Sandstrom, NJ, et al. Female sport participation effect on long-term health-related quality of life. Clin J Sport Med. (2020) 30:526–32. doi: 10.1097/JSM.0000000000000645
82. Proios, M, Athanailidis, I, and Giannitsopoulou, E. The impact of physical activities on the development of the females' character. J Hum Sport Exerc. (2010) 5:485–94. doi: 10.4100/jhse.2010.53.18
83. Younas, A, Zeb, H, Durante, A, and Vellone, E. Sex based differences in depression, anxiety, and quality of life and predictors of quality of life among south Asian individuals with chronic obstructive pulmonary disease: a bayesian analysis. Soc Sci Med. (2024) 351:116989. doi: 10.1016/j.socscimed.2024.116989
84. Kalsoom, U. Gender role in anxiety, depression and quality of life in chronic kidney disease patients: anxiety, depression and QOL in chronic kidney diseases patients. Pak J Med Sci. (2019) 36:869. doi: 10.12669/pjms.36.2.869
85. Aydogan, U, Aydogdu, A, Akbulut, H, Sonmez, A, Yuksel, S, Basaran, Y, et al. Increased frequency of anxiety, depression, quality of life and sexual life in young hypogonadotropic hypogonadal males and impacts of testosterone replacement therapy on these conditions. Endocr J. (2012) 59:1099–105. doi: 10.1507/endocrj.EJ12-0134
86. Liu, Z, Yin, R, Fan, Z, Fan, H, Wu, H, Shen, B, et al. Gender differences in associated and predictive factors of anxiety and depression in people with epilepsy. Front Psych. (2020) 11:670. doi: 10.3389/fpsyt.2020.00670
87. Cui, L, Tang, G, and Huang, M. Expressive suppression, Confucian zhong yong thinking, and psychosocial adjustment among Chinese young adults. Asian J Soc Psychol. (2022) 25:715–30. doi: 10.1111/ajsp.12529
88. Tiggemann, M, and Anderberg, I. Social media is not real: the effect of 'instagram vs reality' images on women's social comparison and body image. New Media Soc. (2020) 22:2183–99. doi: 10.1177/1461444819888720
89. Ong, M, Jaumot-Pascual, N, and Ko, LT. Research literature on women of color in undergraduate engineering education: a systematic thematic synthesis. J Eng Educ. (2020) 109:581–615. doi: 10.1002/jee.20345
90. Valcke, B, Dierckx, K, Van Dongen, S, Van Hal, G, and Van Hiel, A. Participation in extracurricular leisure activities among primary school pupils: effects of ethnic-cultural background, gender and school diversity. J Leis Res. (2023) 54:391–408. doi: 10.1080/00222216.2022.2154181
91. Fusar-Poli, P, Correll, CU, Arango, C, Berk, M, Patel, V, and Ioannidis, JPA. Preventive psychiatry: a blueprint for improving the mental health of young people. World Psychiatry. (2021) 20:200–21. doi: 10.1002/wps.20869
92. Fang, P, Sun, L, Shi, SS, Ahmed Laar, R, and Lu, Y. Influencing factors related to female sports participation under the implementation of Chinese government interventions: an analysis based on the China family panel studies. Front Public Health. (2022) 10:875373. doi: 10.3389/fpubh.2022.875373
93. Kandola, A, Ashdown-Franks, G, Hendrikse, J, Sabiston, CM, and Stubbs, B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. (2019) 107:525–39. doi: 10.1016/j.neubiorev.2019.09.040
94. Alboaneen, D, Pranggono, B, Alshammari, D, Alqahtani, N, and Alyaffer, R. Predicting the epidemiological outbreak of the coronavirus disease 2019 (COVID-19) in Saudi Arabia. Int J Environ Res Public Health. (2020) 17:4568. doi: 10.3390/ijerph17124568
95. Suchting, R, Teixeira, AL, Ahn, B, Colpo, GD, Park, J, and Ahn, H. Changes in brain-derived neurotrophic factor from active and sham transcranial direct current stimulation in older adults with knee osteoarthritis. Clin J Pain. (2021) 37:898–903. doi: 10.1097/AJP.0000000000000987
96. Mei, S, Qin, Z, Yang, Y, Gao, T, Ren, H, Hu, Y, et al. Influence of life satisfaction on quality of life: mediating roles of depression and anxiety among cardiovascular disease patients. Clin Nurs Res. (2021) 30:215–24. doi: 10.1177/1054773820947984
97. Bonsaksen, T. Exploring gender differences in quality of life. Ment Health Rev J. (2012) 17:39–49. doi: 10.1108/13619321211231815
98. Antczak, R, Quashie, NT, Mair, CA, and Arpino, B. Less is (often) more: number of children and health among older adults in 24 countries. J Gerontol B Psychol Sci Soc Sci. (2023) 78:1892–902. doi: 10.1093/geronb/gbad123
99. Kipp, LE, and Bolter, ND. Motivational climate, psychological needs, and personal and social responsibility in youth soccer: comparisons by age group and competitive level. Psychol Sport Exerc. (2020) 51:101756. doi: 10.1016/j.psychsport.2020.101756
100. Schumacher, A, Muha, J, Campisi, SC, Bradley-Ridout, G, Lee, ACH, and Korczak, DJ. The relationship between neurobiological function and inflammation in depressed children and adolescents: a scoping review. Neuropsychobiology. (2024) 83:61–72. doi: 10.1159/000538060
101. Oldehinkel, AJ, Ormel, J, Bosch, NM, Bouma, EMC, Van Roon, AM, Rosmalen, JGM, et al. Stressed out? Associations between perceived and physiological stress responses in adolescents: the TRAILS study. Psychophysiology. (2011) 48:441–52. doi: 10.1111/j.1469-8986.2010.01118.x
102. Madan, S, Savani, K, Mehta, PH, Phua, DY, Hong, Y-Y, and Morris, MW. Stress reactivity and sociocultural learning: more stress-reactive individuals are quicker at learning sociocultural norms from experiential feedback. J Pers Soc Psychol. (2025) 128:1292–314. doi: 10.1037/pspi0000487
103. Zhao, Z, and Gan, Y. Associations between trait mindfulness and physical activity: the parallel mediating effect of exercise positive well-being and exercise psychological distress. BMC Psychol. (2025) 13:418. doi: 10.1186/s40359-025-02751-8
Keywords: physical activity, anxiety, quality of life, gender, adolescents
Citation: Ma S, Gao Y, Zhao L, Sui W, Yang Y and Hu Y (2025) The impact of adolescent physical activity on quality of life: a moderated mediation model. Front. Public Health. 13:1625066. doi: 10.3389/fpubh.2025.1625066
Edited by:
Chin Ngien Siong, Institute of Teacher Education Malaysia Batu Lintang Campus, MalaysiaReviewed by:
Serdar Solmaz, Batman University, TürkiyeMathew Wingerson, University of Colorado Anschutz Medical Campus, United States
Copyright © 2025 Ma, Gao, Zhao, Sui, Yang and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yan Gao, Z2FveWFubHVja0BzZHUuZWR1LmNu